
Pathogenesis.
The extent and severity of esophageal injury due to GER depend on the frequency and the duration of esophageal exposure to the refluxed material, the volume and potency of gastric juice available for reflux, and the ability of the esophageal mucosa to withstand injury and to repair itself.
The pathogenesis of reflux esophagitis or GERD is a multifactorial process. The following factors all contribute to the development of GERD:
Antireflux mechanisms. A positive pressure gradient exists between the abdomen and the thorax. If there were no physiologic barrier at the area of the gastroesophageal junction, GER would occur continuously, especially with increases in intraabdominal pressure or changes in gravitational position and during events associated with abdominal muscle contraction, such as coughing, sneezing, straining, bending, turning in bed, and exercise. The antireflux barrier can be divided into two categories.
Anatomic factors extrinsic to the lower esophageal sphincter (LES) that augment the LES to prevent GER include a distal esophageal mucosal flap, the acute esophagogastric angle, compression of the esophagogastric junction by gastric sling fibers, the diaphragmatic crus acting as pinchcock, a hiatal tunnel, the sling action of the right diaphragmatic crus, and the intraabdominal junction of the esophagus. The longer the intraabdominal segment, the less likely reflux is to occur.
The presence of hiatal hernia with loss of the abdominal esophageal segment supported by the diaphragm and the normal acute esophagogastric angle may lead to GER. However, a direct causal relationship has not been found between hiatal hernia and GER. Nevertheless, a hiatal hernia generally (90%) accompanies reflux esophagitis. It is possible that hiatal hernia enhances the likelihood of LES dysfunction due to the loss of angulation at the esophagogastric junction and the direct transmission of intragastric pressure to the infrathoracic LES. Also, the hiatal hernia may act as a reservoir of refluxate and impair esophageal clearance in the recumbent position, thus promoting esophageal injury.
The closure strength and efficacy of LES
LES corresponds to the 2- to 4-cm zone of asymmetrically thickened smooth muscle at the esophagogastric junction.
LES maintains a high-pressure tone during resting conditions and relaxes with swallowing, esophageal distention, and vagal stimulation. These properties are independent of the diaphragm and persist even when the LES is in the thorax, as in patients with hiatal hernia.
LES is innervated by both excitatory and inhibitory autonomic nerves carried in the vagi to the esophageal plexuses. The major function of the LES inhibitory nerves is to mediate sphincter relaxation in response to swallowing.
LES pressure (LESP) is controlled by neural (most likely cholinergic), hormonal, and myogenic factors.
Resting LES pressure is not constant and varies from minute to minute in the awake state. During sleep, this variability is diminished.
The intrinsic tone (the resting LESP) is one of the major factors that prevent spontaneous GER.
In general, patients with GER have lower LESPs than controls. A minimum resting LESP in the range of 6 to 10 mm Hg prevents GER even during transient increases in intraabdominal pressure.
Changes in resting LES pressure occur throughout the day, especially during the postprandial period. In addition, transient episodes of LES relaxation occur not only in response to swallowing but also spontaneously, a process referred to as inappropriate LES relaxation or transient LES relaxation (TLESR). In physiologic refluxers, most reflux events occur during the relaxation events. In pathologic refluxers (i.e., patients with reflux disease), other mechanisms of reflux also occur, including gradual decreases in resting pressure and episodes of increased intragastric pressure. However, most reflux events continue to occur during TLESR.
TLESR appears to represent a physiologic response to increased gastric distention to relieve intragastric pressure.
Some GER occurs in all individuals with normal or lower-than-normal LESP throughout the day. The frequency of GER increases for 2 hours postprandially. However, patients with esophagitis have significantly more and longer episodes of GER than controls.
Low resting LESP seen in patients with esophagitis may be primary or secondary to injury from reflux and inflammation.
LESP is affected by various drugs and hormones. Avoidance of agents that decrease the LESP and use of agents that increase LESP can be helpful in diminishing GER symptoms and esophageal damage.
Gastric factors
Gastric volume
The occurrence of GER depends on an available reservoir of gastric fluid.
The probability and rate of GER are related to gastric volume.
The rate of reflux and the volume of the refluxate increase with incremental increases in gastric volume, intragastric pressure, and the pressure gradient between the stomach and the esophagus.
Gastric volume is determined by several factors.
Volume and composition of ingested materials.
Rate and volume of gastric secretion.
Rate and efficiency of gastric emptying.
Frequency and volume of duodenogastric reflux.
One or more of the factors in d that favor an increase in gastric volume also favor the occurrence of GER.
Pyloric channel or duodenal ulcers may result in delayed gastric emptying and predispose to increased GER and GERD.
Delayed gastric emptying due to neuromuscular abnormalities such as in collagen vascular diseases, diabetes mellitus, and hypothyroidism or mechanical gastric outlet obstruction may also predispose to GERD.
Irritant potency of the refluxed material
The composition of the material refluxed into the esophagus is important in determining the nature and extent of esophageal injury.
Gastric acid causes esophageal injury by protein denaturation and back diffusion of hydrogen ion into deeper layers of the esophageal wall to cause deeper injury.
Pepsin, a protease, digests esophageal epithelial intercellular substance, causing shedding of epithelial cells.
Duodenogastric reflux, especially postprandially, introduces bile salts and pancreatic enzymes into the stomach, which may then reflux into the esophagus. Bile salts may result in micellar dissolution of the lipids in the esophageal epithelial cell membranes and increase the permeability of the esophageal mucosa to hydrogen ion back diffusion. Pancreatic enzymes may cause proteolytic injury.
Pancreatic digestive enzymes and bile salts may be the significant agents of esophageal injury in patients with gastric hypochlorhydria and near-neutral pH.
Esophageal clearance
The severity of esophageal injury from GER depends on the irritant potency of the refluxed material and its contact time with the esophagus.
The rate of esophageal clearance determines the duration of the exposure of the esophageal mucosa to the refluxed material.
Esophageal clearance of the refluxed material involves three mechanisms:
Volume clearance involves the emptying out of the esophagus of the volume of the refluxed material. It is facilitated by gravity, esophageal motor activity, and salivation.
Normal esophageal motor activity (peristalsis) is required for esophageal clearance.
Primary peristalsis is initiated by swallowing, and the contraction wave progresses in a sequential fashion throughout the entire length of the esophagus, resulting in esophageal emptying into the stomach. Normally, primary peristalsis occurs about once a minute while an individual is awake. It is the main esophageal motor event that clears the esophagus of refluxed material. The absence of swallowing and esophageal peristalsis during sleep impedes esophageal clearance of refluxed material and predisposes to esophageal injury. Similarly in patients with abnormal esophageal motility, increased nonperistaltic contractions lead to increased reflux injury to the esophagus.
Secondary peristalsis is elicited with distention of the esophagus by a bolus of food or refluxed fluid. It has a limited effect on volume clearance, because it does not result in a complete stripping peristaltic wave.
Acid clearance involves the disappearance of the hydrogen ion from the esophageal mucosa after the reflux of acid fluid. It is accomplished by a neutralizing action of swallowed saliva.
Saliva is the third factor that contributes to esophageal clearance.
Normal awake individuals generate 0.5 mL of saliva per minute.
Salivation stops during sleep.
Salivation stimulates swallowing.
Stimuli that increase salivary secretion include sucking, eating, intubation, and cholinergic agents.
Under basal conditions, saliva has a pH of 6 to 7 due to the presence of bicarbonate ion as the major buffer.
During stimulation, both the salivary volume and the bicarbonate ion concentration increase.
Normal salivary flow effectively neutralizes small volumes (-1 mL) of refluxed acid.
Salivation, by promoting swallowing and primary stripping peristalsis, clears the esophagus of the main volume of the refluxed material. Subsequently saliva itself clears the acid from the esophageal mucosa by its neutralizing action.
Diminished salivation, primary (e.g., in Sjogren's syndrome) or secondary (e.g., due to anticholinergic drugs), causes delayed acid clearance and promotes esophageal injury.
Tissue resistance of the esophageal mucosa.
The esophageal mucosa itself has intrinsic protective mechanisms that resist and limit mucosal injury.
Preepithelial defenses
The luminal surface of esophageal epithelium is lined by a layer of mucus that serves as both a lubricant and a protective barrier against noxious and irritant luminal contents. This viscous gel layer prevents large protein molecules like pepsin from contacting the underlying epithelium directly and slows down hydrogen ion back diffusion.
Underneath the mucous layer, there is an area of low turbulence called the unstirred water layer, which is rich in bicarbonate. This layer establishes a protective alkaline microenvironment on the epithelial surface, neutralizing the hydrogen ion that penetrates the mucous layer.
Mucus and bicarbonate are secreted by salivary glands and submucosal glands located just below the upper esophageal sphincter and near the esophagogastric junction. The rate of secretion of these glands increases with vagal stimulation and with prostaglandins.
Postepithelial defenses. As in all tissues, adequate blood flow and normal tissue acid-base status are essential for the maintenance of a healthy epithelium. Blood flow provides the epithelium with oxygen, nutrients, and bicarbonate (HCO3-) as buffer and removes injurious waste products.
Epithelial regeneration.
Despite the intrinsic ability of the esophageal mucosa to resist injury, prolonged exposure to noxious substances results in epithelial cell necrosis. Cell death further increases epithelial permeability, setting up a vicious circle for further damage. The replicating cells of the stratum basale along the basement membrane need to be protected for epithelial regeneration. The destruction of this layer appears to be necessary for the development of esophageal ulcers, strictures, and Barrett's epithelium. There is evidence that epithelial cell turnover and replication is increased after hydrogen (H+) injury. Basal cell hyperplasia seen in mucosal biopsies of patients with reflux esophagitis lends further support to this finding. Normal turnover rate for esophageal epithelium is 5 to 8 days. This rate seems to be increased to 2 to 4 days with injury. This will allow for epithelial renewal and repair in a short time if further injury is prevented.
A history of recurrent heartburn along with a positive response to antacids or acid-suppressing medication is adequate to diagnose Acid Reflux Disease. Specific testing is reserved for patients who have (1) Acid Reflux Disease plus alarm symptoms of dysphagia, weight loss, or gastrointestinal bleeding; (2) Acid Reflux Disease of sufficient chronicity (e.g., 5 years) to raise concern for Barrett's esophagus; and (3) suspected Acid Reflux Disease with atypical symptoms, such as chest pain or oropharyngeal, laryngeal, or airway symptoms.
Establishing Acid Reflux Disease as a Cause of Nonheartburn Symptoms
Currently, the preferred method for establishing Acid Reflux Disease as the cause of symptoms (e.g., chest pain, wheezing) is an empirical trial of acid suppression with a PPI (e.g., omeprazole, 20 mg twice daily), which normalizes esophageal acidity in approximately 95% of subjects. In some instances, a bedtime dose of a histamine H2-receptor antagonist (e.g., ranitidine, 300 mg) is added to reduce the possibility of nocturnal acid breakthrough. The treatment period in which to expect a satisfactory response is 2 to 4 weeks for chest pain and 2 to 3 months for inflammatory disease of the airway. Resolution of the symptoms supports Acid Reflux Disease as possibly causal. Confirmation may be obtained by relapse when medication is withdrawn and by a subsequent positive response to re-treatment, as confirmed by documenting control of esophageal acidity on pH monitoring while undergoing PPI therapy. Failure of symptoms to improve with PPI therapy is not generally an indication for antireflux surgery (see later) but rather an indication to search for another disease. A rarely used alternative is the Bernstein test, in which acid (0.1 N HCl, pH 1.1) or saline (control) is perfused through a catheter positioned in the midesophagus. If symptoms typical of those that occur spontaneously develop with acid but not saline, the test is considered positive for Acid Reflux Disease.
Tests for Reflux
Documenting acid reflux is not necessary except when symptoms fail to respond to PPI therapy or when surgery is being considered. Esophageal pH monitoring, the “gold standard” for identifying acid reflux, is performed by fixing a small pH probe in the esophagus, 5 cm above the LES, and recording all episodes in which esophageal pH drops to less than 4 over a 24- to 48-hour period. The number and duration of each acidic event, when combined, yield a value for total esophageal acid contact time. Total acid contact times of greater than 5% are abnormal and consistent with a diagnosis of Acid Reflux Disease. An event marker activated by the patient also allows symptoms to be related to episodes of esophageal acidity. An upper gastrointestinal series can detect grossly abnormal reflux by observing movement of barium from the stomach to the esophagus with the patient in the head-down position. It has low sensitivity but, when positive, has high predictive value. The positive predictive value is much lower, however, if reflux is induced by having the subject sip water through a straw in the head-down position. This test is rarely useful for therapeutic decisions.
Tests for Esophageal Injury
Endoscopic signs.
Tests of Esophageal Motor Function
An upper gastrointestinal series or barium swallow is valuable for identifying gross reflux and marked abnormalities in esophageal anatomy (e.g., hiatal hernia, diverticulum) and peristaltic and sphincter function. More subtle abnormalities, however, require esophageal manometry. Low mean LES pressure (<10 mm Hg) is a specific but insensitive marker of Acid Reflux Disease, with 60% of patients having normal values. Currently, the major uses of esophageal manometry in Acid Reflux Disease are to (1) position the pH probe for reflux testing, (2) exclude motor disease (achalasia, scleroderma), and (3) quantify peristaltic amplitudes before surgical fundoplication. If contraction amplitudes average less than 30 mm Hg, a partial (Toupet) rather than complete (Nissen) wrap may be preferable to avoid postoperative dysphagia.
Recurrent heartburn, when properly defined, is the hallmark of Acid Reflux Disease and enables the diagnosis to be made by the history alone. The heartburn associated with Acid Reflux Disease typically occurs once or twice per day and lasts from a few minutes to an hour or more if untreated. This pattern recurs, but with considerable variation in frequency and severity. However, neither the frequency, severity, nor duration of heartburn predicts disease severity on endoscopy. Acid Reflux Disease can also be associated with dysphagia, an alarm symptom because it raises concern for the presence of a peptic stricture or adenocarcinoma arising in Barrett's esophagus. For this reason, dysphagia is an indication for early endoscopy.
The damage in Acid Reflux Disease is best assessed by upper endoscopy and esophageal biopsy. Endoscopy may reveal friability, erosions, ulcers, strictures, or Barrett's esophagus in a third of subjects. In the other two thirds, endoscopic findings are normal but esophageal biopsy may show basal cell hyperplasia, elongation of the rete pegs, inflammatory cell infiltrates, cell edema, dilated intercellular spaces in squamous epithelium, or any combination of these findings. “Dilated intercellular spaces” is the earliest detectable lesion in NERD and correlates with heartburn because it reflects “leakiness” of the paracellular pathway to refluxed gastric acid. A barium swallow or upper gastrointestinal series may also detect ulcers, strictures, and hiatal hernias, but it does not reliably detect inflammation, erosions, or Barrett's esophagus.
Although Acid Reflux Disease is often used synonymously with reflux damage to the esophagus, Acid Reflux Disease includes reflux damage to the oropharynx, larynx, and respiratory tract. Consequently, symptoms and signs of Acid Reflux Disease can include sore throat/pharyngitis, earache/otitis, eroded tooth enamel, hoarseness/laryngitis, bronchitis/chronic cough, asthma/wheezing, and aspiration pneumonia. With the exception of pneumonia, which occurs as a result of gross regurgitation and aspiration of mixed gastric content, damage to the oropharynx, larynx, and airways is mediated by refluxed gastric acid. Asthma (wheezing) and bronchitis (chronic cough) can be triggered either directly by contact of acid with airway epithelium (microaspiration) or indirectly through an esophagopulmonary vagal reflex initiated by contact of acid with esophageal epithelium. The frequency with which Acid Reflux Disease causes, as opposed to being caused by, wheezing/asthma, chronic cough/bronchitis, and hoarseness/laryngitis is unknown.
Associated Conditions
Acid Reflux Disease can develop as a consequence of other conditions, such as Zollinger-Ellison syndrome, scleroderma, diabetes mellitus, nasogastric intubation, and pregnancy.
Gastroesophageal reflux is a physiologic process that refers to the effortless movement of stomach contents from the stomach to the esophagus. It occurs in everyone, multiple times every day, usually without producing symptoms or signs of damage. Reflux can also be pathologic and produce symptoms and signs of injury to the esophagus, oropharynx, larynx, and respiratory tract. Reflux damage to the esophagus (reflux esophagitis) is the most common form of Acid Reflux Disease and is most often recognized by recurrent heartburn. In almost all patients with heartburn, esophageal mucosal pathology is identifiable, although only about 40% have endoscopically detectable erosions. The remaining 60% of patients with heartburn have endoscopically undetectable (microscopic) pathology—termed nonerosive reflux disease (NERD).
Acid Reflux Disease is one of the most common diseases in the Western world based on the prevalence of heartburn. In the United States, about 45% of adults have heartburn at least once a month, about 20% once a week, and about 10% daily. Heartburn affects men two- to threefold more often than it affects women and is more common in whites than blacks. Although Acid Reflux Disease rarely causes death, it reduces quality of life and has a morbidity rate of 10 to 15% secondary to ulceration, bleeding, stricture, Barrett's esophagus, and adenocarcinoma. The overall risk for esophageal adenocarcinoma in patients with heartburn is very low, with estimates of 1 in 2500 cases per year for those with daily heartburn to 1 in 10,000 cases per year for those with monthly heartburn.
Acid Reflux Disease develops when acidic stomach contents reflux into the esophagus and remain there long enough to overcome the resistance of the esophageal epithelium. Based on 24-hour esophageal pH monitoring, Acid Reflux Disease develops in at least two fundamentally different ways: (1) under conditions in which there is prolonged contact of the esophageal epithelium with refluxed stomach acid and (2) under conditions in which the esophageal epithelium is damaged despite a normal duration of contact with refluxed stomach acid. Prolonged acid contact results from defects in the antireflux barriers or luminal clearance mechanisms (or both), with transient LES relaxations accounting for more than 50% of acid reflux events in NERD. These relaxations are non–swallow-induced, reflex relaxations of the LES caused by stomach fundic distention. They are associated with acid reflux because they are twice as long as relaxations with swallowing and, unlike swallow-induced LES relaxations, are accompanied by inhibition of diaphragmatic contraction and unaccompanied by lumen-obliterating esophageal peristalsis. The cause of the increase in the frequency of acid reflux episodes associated with transient relaxations in patients with Acid Reflux Disease is unclear but is unrelated to delayed stomach emptying or infection with Helicobacter pylori. A diet rich in nonabsorbable carbohydrates may be one possible provocateur. In erosive esophagitis, transient LES relaxations account for less than 50% of acid reflux events, with most occurring across a mechanically weak LES. Whether LES weakness causes erosive esophagitis or is a consequence of it remains unclear because products released during inflammation can impair LES contractility. Similarly, hiatal hernias and impaired peristalsis are common in erosive esophagitis, but whether they are cause or consequence is also unclear because esophagitis can result in both esophageal shortening (by sustained contraction of the longitudinal muscle) and peristaltic dysfunction (by weakening circular muscle contractility). Patients with heartburn despite normal acid contact time presumably have primary defects in tissue resistance, with these defects probably being acquired by dietary indiscretions such as excess exposure to alcoholic, hypertonic, or hot-temperature products.
Gastroesophageal reflux disease (GERD) is defined as symptoms or tissue damage resulting from reflux of gastric acid into the esophagus and more proximal structures.
The predominant symptoms of GERD are heartburn and regurgitation.
Atypical symptoms include cough, asthma, hoarseness, chest pain, hiccups, and dental erosions.
Symptom response to a therapeutic trial of PPIs can be diagnostic.
Endoscopic evaluation is recommended for patients with warning symptoms of dysphagia, odynophagia, early satiety, weight loss, or bleeding, and atypical symptoms (cough, asthma, hoarseness, chest pain, aphthous ulcers, hiccups, dental erosions).
Patients with symptoms refractory to empiric acid suppression or requiring continuous medication for prolonged periods should also undergo endoscopy.
Ambulatory pH monitoring is used to establish elevated esophageal acid exposure and symptom-reflux correlation in patients with ongoing symptoms despite acid suppression (especially if endoscopy is negative) or those with atypical symptoms. It is also used to determine adequacy of acid suppression in patients with established GERD and ongoing symptoms.
Lifestyle Modification
The basics of lifestyle modification include eating small meals; refraining from eating for 2-3 hours before lying down; elevating the head of the bed 4-6 in.; decreasing intake of fatty foods, chocolate, coffee, cola, and alcohol; and smoking cessation.
Lifestyle modification also includes avoiding medications such as calcium channel blockers, theophylline, sedatives/tranquilizers, and anticholinergics, as they may potentiate reflux.
Lifestyle modifications alone are unlikely to resolve symptoms in the majority of GERD patients, but should be recommended in conjunction with medications.
Medications
In patients with mild or intermittent symptoms, over-the-counter antacids and H2RAs can be used intermittently or prophylactically if necessary.
PPIs have been demonstrated to be more effective than placebo or standard-dose H2RA in symptomatic relief as well as endoscopic healing of GERD. Higher doses (omeprazole, 20–40 mg PO bid or equivalent) may be required in severe esophagitis or persistent symptoms. Continuous long-term PPI therapy is safe and effective in maintaining remission of GERD symptoms, and is recommended for patients with erosive esophagitis, Barrett's esophagus, and severe symptoms.
Standard doses of H2RAs can result in symptomatic benefit in up to 60% of patients and endoscopic healing in 50%. Higher doses of H2RAs (equivalent to ranitidine, 600 mg daily) improve the healing rate to 75% at a higher cost. Dosage adjustments are required in renal insufficiency.
Surgery
Indications for fundoplication include the need for continuous or increasing doses of medication in patients who are good surgical candidates. Patients who require aggressive long-term medical therapy should be offered the surgical option. Other indications include patient preference for surgery and noncompliance with medical therapy.
The success rate of laparoscopic fundoplication in controlling GERD symptoms exceeds 90%, with fewer complications compared to the open technique. Elevated esophageal acid exposure and correlation of symptoms to reflux events on ambulatory pH monitoring predict a higher likelihood of a successful outcome.
Patients with medical treatment failures need careful evaluation to determine whether symptoms are indeed related to acid reflux before surgical options are considered; these patients often have other diagnoses including visceral hypersensitivity and functional heartburn.
Complications
Esophageal ulceration and stricture formation can occur in patients with GERD. Iron-deficiency anemia is less common.
GERD can contribute to laryngitis, laryngeal ulcers, asthma, and dental caries.
Barrett's esophagus is a change in the esophageal mucosa from normal squamous epithelium to specialized intestinal metaplastic epithelium due to longstanding acid related injury. It carries a small risk of progression to esophageal adenocarcinoma. Endoscopic surveillance for Barrett's esophagus should be considered in patients with a symptom history that exceeds 5 years.
The history and clinical manifestations of Acid Reflux Disease are the most important diagnostic aids; objective testing can quantify the extent and severity of the process. In the vast majority of sufferers, typical symptoms of Acid Reflux Disease and the response to initial gastric acid suppressive therapy make the diagnosis relatively easy. Diagnostic evaluation becomes important when symptoms are atypical and/or do not respond to therapy.
DOCUMENTING REFLUX.
Reflux during a barium swallow in adults is uncommon unless vigorous provocative maneuvers are employed. When spontaneous reflux of barium is seen, it usually denotes free reflux. The absence of reflux seen radiographically does not, however, imply that the sufferer does not have Acid Reflux Disease.
The 24-hour monitoring of esophageal pH can be performed with a portable unit, which allows the sufferer to follow an almost normal lifestyle. During the prolonged monitoring period, the relationship between symptoms (heartburn, chest pain, wheezing) and episodes of acid reflux can be ascertained, and calculations can be made of the number of episodes of reflux and the amount of time the esophagus is acidified (pH - 4). A small amount of reflux, especially in the postprandial period, can be seen normally. Repeated and prolonged bursts of acid exposure suggest that abnormal gastroesophageal reflux is present.
In children and infants, reflux can be measured noninvasively by scanning the esophageal area with a gamma-camera after placing a solution of 99m Tc sulfur colloid in the stomach. An abdominal binder is used to increase intra-abdominal pressure and to stress the gastroesophageal junction if free reflux is not seen.
LINKING REFLUX TO SYMPTOMS.
If pain is the predominant symptom, rather than heartburn, a Bernstein test may be performed using the same catheter as is used for esophageal manometry. After a 5-minute period of dripping normal saline in the mid-esophagus, the infusion is changed to 0.1 N hydrochloric acid. Reproduction of the symptoms during acid infusion (usually 4 to 5 minutes into the infusion), followed by rapid symptom disappearance after returning to a saline infusion, suggests an esophageal cause of the discomfort.
As another approach, the sufferer is asked to signal the time of discomfort during prolonged pH monitoring of the esophagus. If the sufferer signals discomfort at the same time that acid reflux is demonstrated by the pH probe, then a causal relationship is more likely.
ASSESSING THE EFFECT OF REFLUX ON THE ESOPHAGEAL MUCOSA.
A barium swallow detects gross changes, such as stricture formation or a deep esophageal ulcer, but misses the much more common shallow ulcerations and erosions, which are detected by endoscopy. Only discrete lesions such as erosions and ulcerations should be taken as proof of esophageal damage, because endoscopic findings, such as erythema, edema, or friability, are subject to wide interobserver variation. In approximately one-half of sufferers with moderate to severe symptoms of Acid Reflux Disease, the mucosa appears absolutely normal, but a biopsy may demonstrate the histologic changes of reflux.
APPROACH
Endoscopy is generally indicated if symptoms are prolonged and do not respond to empiric treatment, or if systemic manifestations, such as weight loss, anemia, and occult blood-positive stool are present. If the appearance of the esophageal mucosa is normal during endoscopy, biopsies can also be obtained to search for objective evidence of microscopic esophagitis. If dysphagia is present, a barium swallow is appropriate. Uncommonly, reflux is demonstrated, a stricture found, or a deep ulcer seen, which leads to immediate endoscopy for more complete evaluation. After first evaluation, it may be appropriate to begin empiric therapy (see Treatment, below). If the response to therapy is poor, esophageal pH monitoring can confirm the diagnosis. At the same time, esophageal manometry may be performed to estimate LES pressure and to determine the presence or absence of peristaltic waves.
Prevention of retrograde flow of gastrointestinal contents is a major function of the lower esophageal sphincter (LES) . Retrograde flow is prevented by the lower esophageal sphincters, which remain closed between swallows.
The lower esophageal sphincter is composed of smooth muscle and is innervated by parallel sets of parasympathetic excitatory and inhibitory pathways. It remains closed because of its intrinsic myogenic tone, which is modulated by the excitatory and inhibitory nerves. It opens in response to the activity of the inhibitory nerves. The neurotransmitters of the excitatory nerves are acetylcholine and substance P, and those of the inhibitory nerves are vasoactive intestinal peptide (VIP) and nitric oxide. The function of the LES is supplemented by the striated muscle of the diaphragmatic crura, which surrounds the LES and acts as an external LES. Relaxation of the LES without esophageal contraction occurs during belching and gastric distention. Gastric distention-evoked transient lower esophageal sphincter relaxation (tLESR) is a vasovagal reflex. Fatty meals, smoking, and beverages with a high xanthine content (tea, coffee, cola) also cause a reduction in sphincter pressure. Many hormones and neurotransmitters can modify LES pressure. Muscarinic M2 and M3receptor agonists, a-adrenergic agonists, gastrin, substance P, and prostaglandin F2acause contraction. Nicotine, b-adrenergic agonists, dopamine, cholecystokinin, secretin, VIP, calcitonin gene-related peptide (CGRP), adenosine, prostaglandin E, and nitric oxide donors such as nitrates reduce sphincter pressure.
Antegrade esophageal flow is achieved by the act of swallowing with the initiation of primary peristalsis. Gastroesophageal reflux is prevented by the physiologic lower esophageal sphincter (LES).
When the LES fails to function as an effective barrier to reflux, gastroesophageal reflux develops, with the associated complications of mucosal inflammation (reflux esophagitis).
Gastroesophageal reflux disease (GERD) refers to the varied clinical manifestations of reflux of stomach and duodenal contents into the esophagus and is preferable to the term "reflux esophagitis." Although GERD may be associated with a sliding hiatal hernia, the term "symptomatic hiatal hernia" tends to emphasize an anatomic entity and not the underlying pathophysiology. GERD can be characterized by any combination of symptoms and radiologic, endoscopic, or pathologic changes. In its milder manifestations, it is a common disease; its most florid state is uncommon but may be life-threatening.
HEARTBURN
Heartburn is the most common manifestation of esophageal disease and may occur in up to 20% of the population. The term "burning" rather than "pain" is usually used, although heartburn can increase in intensity until it is perceived as chest pain. Patients often illustrate heartburn with a movement of the open hand up and down the sternum, as compared with the stationary, tightly clenched fist of angina pectoris. Heartburn is usually relieved, even if only temporarily, by taking antacids. A constant burning unrelieved by antacids may well be of esophageal origin, but it does not represent heartburn. Heartburn is often worse after recumbency or lifting and may follow overeating or alcoholic indiscretion.
REGURGITATION
Regurgitation of fluid contents into the mouth often accompanies heartburn. Sometimes regurgitation is associated with eructation; often it accompanies bending over, lifting, or lying down at night. The bitter regurgitated fluid is often described as yellow-brown or green. Regurgitation at night may lead to stridor or to wheezing, a hoarse voice, and other respiratory symptoms from unrecognized reflux.
SPONTANEOUS ESOPHAGEAL CHEST PAIN
In addition to the discomfort from severe reflux, which can advance from heartburn into pain, abnormal contractile activity of the esophageal muscle can cause severe chest pain that is clinically indistinguishable from angina pectoris in terms of intensity, radiation, relationship to exercise, and even response to nitroglycerin. pain of esophageal origin can radiate directly through to the back and is often found in patients who also have dysphagia. Esophageal chest pain can last from several seconds to many hours.
REFLUX ESOPHAGITIS
Reflux of stomach contents into the lower esophagus is the first and foremost cause of esophagitis. Many causative factors are involved, less well characterized than the name implies:
Decreased efficacy of esophageal antireflux mechanisms, particularly LES tone. Central nervous system depressants, hypothyroidism, pregnancy, systemic sclerosing disorders, alcohol or tobacco exposure, or the presence of a nasogastric tube may be contributing causes. In most instances, no antecedent cause is identified.
Presence of a sliding hiatal hernia.
Inadequate or slowed esophageal clearance of refluxed material.
Delayed stomach emptying and increased stomach volume, contributing to the volume of refluxed material.
Reduction in the reparative capacity of the esophageal mucosa by protracted exposure to stomach juices.
Any one of the aforementioned influences may assume primacy in an individual case, but more than one is likely to be involved in most instances. The acid-peptic action of stomach juices is critical to the development of esophageal mucosal injury; in severe cases, refluxed bile from the duodenum also may contribute to the mucosal disruption.
MORPHOLOGY.
The anatomic changes depend on the causative agent and on the duration and severity of the exposure. Simple hyperemia ( redness) may be the only alteration. In uncomplicated reflux esophagitis, three histologic features are characteristic
1. The presence of inflammatory cells, including eosinophils, neutrophils, and excessive numbers of lymphocytes, in the epithelial layer
2. Basal zone hyperplasia exceeding 20% of the epithelial thickness
3. Elongation of lamina propria papillae with congestion, extending into the top third of the epithelial layer
Infiltrates of intraepithelial eosinophils are believed to be an early histologic abnormality, since they occur even in the absence of basal zone hyperplasia. Intraepithelial neutrophils are markers of more severe injury, such as ulceration, rather than reflux esophagitis per se.
Clinical Features.
Although largely limited to adults over age 40, reflux esophagitis is occasionally seen in infants and children. The clinical manifestations consist principally of dysphagia; heartburn; and sometimes regurgitation of a sour brash, hematemesis, or melena. The severity of symptoms is not related closely to the presence or degree of histologic esophagitis; most people experience reflux symptoms without damage to the distal esophageal mucosa, owing to the short duration of the reflux. Anatomic damage appears best correlated with prolonged exposure of the lower esophagus to refluxed material. Rarely, chronic symptoms are punctuated by attacks of severe chest pain that may be mistaken for a heart attack. The potential consequences of severe reflux esophagitis are bleeding, development of stricture, and a tendency to develop Barrett esophagus, with its attendant risks.
Several factors must work in concert to produce clinical effects of esophageal reflux. Normal subjects may have a few short-duration reflux episodes postprandially and in the upright position. Those in whom reflux has produced symptoms or pathologic changes will demonstrate more frequent and prolonged episodes of reflux, which also tend to occur at night. The factor or factors that cause this difference are not entirely known. However, important differences between persons with and without reflux might help explain these findings.
The LES is a specialized bundle of circular muscle at the lower end of the esophagus with different physical and pharmacologic characteristics when compared with the circular muscle above and below it. Although mean LES pressure is significantly lower in subjects with GERD than in normal persons, much overlap occurs between the groups; LES pressure is not very useful in predicting whether reflux is present in an individual patient unless the pressure is very low. The most common event associated with reflux appears to be a transient relaxation of the LES unassociated with either swallowing or the distention of the esophageal body by refluxed fluid. Thus, two abnormalities of LES may be associated with reflux: a sphincter with very low tone, as measured by LES pressure, or inappropriate relaxation of a normally competent sphincter.
Several factors are important in removing refluxed material from the esophagus. The upright position facilitates esophageal emptying by gravity. Peristaltic waves initiated by swallowing or by esophageal distention help remove the refluxed material. Acid placed within the esophagus is cleared less well by patients with GERD than by normal subjects, although the manometric tracings seen in both groups seem identical. Clearing of acid regurgitation occurs in two phases: the bulk of the fluid is returned to the stomach by a peristaltic contraction, and the remaining acid film clinging to the esophageal wall is neutralized by swallowed saliva.
The composition and perhaps the quantity of the refluxed material also play a role in the production of GERD. Gastric acid and pepsin seem clearly important in the pathogenesis of GERD. Bile salts, and possibly pancreatic enzymes, may be responsible in patients in whom acid is absent. The combination of bile salts plus acid is more injurious to the esophagus than either agent alone. Other less well-studied factors, such as altered or abnormal esophageal mucus, swallowed saliva of high bicarbonate content, and diminished resistance of the esophageal mucosa to digestion, may be important in determining the amount of mucosal damage in GERD.
Esophageal squamous epithelium reacts to reflux by an increase in the basal cell or germinative layer. The dermal pegs are increased in height and may become more vascular. If the process becomes more severe, the epithelial layer is destroyed, with the appearance of micro-ulcers and classic signs of inflammation in the lamina propria, such as infiltration with polymorphonuclear leukocytes and edema. Even deeper lesions cause first submucosal and then muscular inflammation and fibrosis, resulting in an esophageal stricture. Why reflux is so common, yet inflammation and stricture formation are relatively uncommon, is not known.
Reflux during pregnancy, once thought to be due to the increased abdominal pressure from the fetus, may be due mainly to diminished LES strength caused by increased estrogen and progesterone. Weight gain also tends to aggravate reflux through an unknown mechanism. Resection of the lower esophageal area for cancer or myotomy for achalasia can lead to severe postoperative reflux. Gastroesophageal reflux with stricture formation is especially severe in patients with progressive systemic sclerosis.
The crural diaphragm usually wraps around the gastroesophageal junction to augment the intrinsic LES. In a hiatal hernia, an anatomic displacement of the LES and crural diaphragm is seen. Although hiatal hernias may be associated with reflux, the presence of a hiatal hernia is now considered to be much less of a factor in GERD than previously thought, because it is present in a large percentage of normal subjects. It is not appropriate to spend time trying to define whether a hiatal hernia is present or absent in dealing with most patients with GERD; rather, the focus should be on the symptoms of reflux.
GASTROESOPHAGEAL REFLUX DISEASE
Pathophysiology: The normal antireflux mechanisms consist of the LES, the crural diaphragm, and the anatomic location of the gastroesophageal junction below the diaphragmatic hiatus. Reflux occurs only when the gradient of pressure between the LES and the stomach is lost. It can be caused by a sustained or transient decrease in LES tone. A sustained hypotension of the LES may be due to muscle weakness that is often without apparent cause. Secondary causes of LES incompetence include scleroderma-like diseases, myopathy associated with chronic intestinal pseudo-obstruction, pregnancy, smoking, anticholinergic drugs, smooth-muscle relaxants [b-adrenergic agents, aminophylline, nitrates, calcium channel blockers, phosphodiesterase inhibitors that increase cyclic AMP or cyclic GMP (including sildenofil)], surgical destruction of the LES, and esophagitis.tLESRwithout associated esophageal contraction is due to a vagal reflex in which LES relaxation is elicited by gastric distention. Increased tLESR is associated with GERD. A similar reflex operates during belching. Apart from incompetent barriers, gastric contents are most likely to reflux (1) when gastric volume is increased (after meals, in pyloric obstruction, in gastric stasis, during acid hypersecretion states), (2) when gastric contents are near the gastroesophageal junction (in recumbency, bending down, hiatus hernia), and (3) when gastric pressure is increased (obesity, pregnancy, ascites, tight clothes). Incompetence of the diaphragmatic crural muscle, which surrounds the esophageal hiatus in the diaphragm and functions as an external LES, also predisposes to GERD.
Reflux esophagitis is a complication of reflux and develops when mucosal defenses are unable to counteract the damage done by acid, pepsin, and bile. Mild esophagitis involves microscopic changes of mucosal infiltration with granulocytes or eosinophils, hyperplasia of basal cells, and elongation of dermal pegs. Endoscopic appearance may be normal. Erosive esophagitis involves endoscopically apparent mucosal damage, redness, friability, bleeding, superficial, linear ulcers, and exudates. Peptic stricture results from fibrosis that causes lumenal constriction. These strictures occur in ~10% of patients with untreated GERD. Short strictures caused by spontaneous reflux are usually 1 to 3 cm long and are present in the distal esophagus near the squamocolumnar junction. Long, tubular peptic strictures can result from persistent vomiting or prolonged nasogastric intubation. Erosive esophagitis may cause bleeding and heal by intestinal metaplasia (Barrett's esophagus) that is a risk factor for adenocarcinoma.
Clinical Features: Regurgitation of sour material in the mouth and heartburn are the characteristic symptoms of GERD. Heartburn is produced by the contact of refluxed material with the inflamed or sensitized esophageal mucosa. Angina-like or atypical chest pain occurs in some patients, while others experience no heartburn or chest pain. Persistent dysphagia suggests development of a peptic stricture. Most patients with peptic stricture have a history of several years of heartburn preceding dysphagia. However, in one-third of patients, dysphagia is the presenting symptom. Rapidly progressive dysphagia and weight loss may indicate the development of adenocarcinoma in Barrett's esophagus. Bleeding occurs due to mucosal erosions or Barrett's ulcer. Severe reflux may reach the pharynx and mouth and result in laryngitis, morning hoarseness, and pulmonary aspiration. Recurrent pulmonary aspiration can cause aspiration pneumonia, pulmonary fibrosis, or chronic asthma. By contrast, many patients with GERD remain asymptomatic or self-treated and do not seek attention until severe complications occur.
TREATMENT OF GASTROESOPHAGEAL REFLUX DISEASE (GERD)
Most mildly symptomatic patients with reflux and some moderately afflicted individuals can be helped by simple measures designed to alter the frequency or type of esophageal reflux. Elevating the head of the bed by 6 to 8 inches is a simple and effective form of therapy. Esophageal pH monitoring has shown that this simple measure decreases the frequency and length of reflux episodes. Pillows to elevate the thorax do not work well, as patients tend to roll off the pillows during the night. A foam rubber wedge can be used if the bed frame cannot be moved. Avoiding food and fluid for at least 3 hours before retiring decreases the amount of material available for reflux at night. Avoiding food that the patient finds distressing and that may decrease LES pressure, such as fatty foods, chocolate, and onions, makes sense but has never been subjected to clinical trial. Acid can be neutralized by taking 30 mL of aluminum hydroxide-magnesium hydroxide antacid 1 and 3 hours after meals and at bedtime, but most patients do not tolerate frequent antacid administration. An attempt should be made to have the patient stop smoking, drinking alcohol, and overeating.
If these simple measures are not effective, systemic medical treatment is indicated. The H2 -receptor antagonists in the usual dosage range for duodenal ulcer and titrated to the individual patient improve heartburn better than placebo. An increased frequency of administration and/or higher dosage regimens--cimetidine, 800 mg; ranitidine, 300 mg; or famotidine, 40 mg (each twice per day)--are more effective for controlling symptoms and healing peptic esophagitis, which usually requires 12 weeks.
The proton-pump inhibitors omeprazole (20 mg/day) or lansoprazole (30 mg/day) can give dramatic symptom relief and heal esophagitis in 4 to 8 weeks. Proton-pump inhibitors are usually the treatment of choice for mucosal disease, especially moderate to severe esophagitis seen endoscopically.
Prokinetic agents may also be useful in the treatment of GERD symptoms with no to mild esophagitis, occasionally in addition to gastric acid suppressants. Metoclopramide, 10 mg given three times a day, can be helpful, but CNS side effects can occur in 25% of cases and may limit its usefulness.
Summary:
Step 1. Simple measures (lifestyle changes , dietary modifications and OTC antacids)
A. Elevate head of bed
B. Avoid food and fluid intake before bedtime
C. Avoid cigarettes, coffee, alcohol
D. Avoid chocolate, peppermint
E. Avoid tight clothing around the waist
F. Take antacids 1 hour after meals, at bedtime, and as needed
G. Reduce fat in diet
H. Lose weight
Step 2a.H2 -receptor antagonists
A. Cimetidine, 300 mg q.i.d.
B. Ranitidine, 150 mg b.i.d.
C. Famotidine, 20 mg b.i.d.
D. Nizatidine, 150 mg b.i.d.
Step 2b. Prokinetic agents
Metoclopramide, 10 mg q.i.d.
Step 3. Measures for patients with GERD resistant to H2 -receptor antagonists
Proton pump inhibitor: omeprazole, 20 mg/day, or lansoprazole, 30 mg/day
Step 4. Measures for patients with GERD resistant to steps 1, 2, and 3 or patients who need long-term maintenance treatment
Surgical fundoplication
Once healing of esophagitis has been achieved with either an H2 -antagonist or a proton-pump inhibitor, recurrence rates exceed 80% if no maintenance therapy is used. Maintenance therapy for esophagitis generally requires full dosage of an H2 -receptor antagonist or a proton-pump inhibitor.
The most thoroughly evaluated classification scheme for esophagitis is the Los Angeles system, which categorizes mucosal injury as grade A, B, C, or D. However, it is important to note that the Los Angeles system does not consider strictures, hiatal hernia, or Barretts metaplasia; the endoscopist is required to describe these separately.
Los Angeles Endoscopic Grading Scheme for Esophagitis Severity
Grade A
One (or more) mucosal breaks no longer than 5 mm that do not extend between the tops of two mucosal folds.
Grade B
One (or more) mucosal breaks more than 5 mm long that do not extend between the tops of two mucosal folds.
Grade C
One (or more) mucosal breaks that are continuous between the tops of two or more mucosal folds but involve lesser than 75% of the circumference.
Grade D
One (or more) mucosal breaks that involve at least 75% of the esophageal circumference.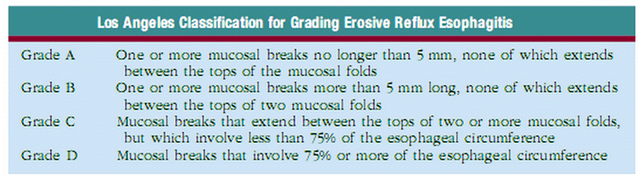



{kind=link}
What is acid reflux disease? An acid reflux flash animation that simply answers frequently asked questions about GERD and Acid Reflux Surgery.
Acid Reflux Disease Complications
Hemorrhage and Perforation
Hemorrhage and esophageal perforation are rare complications of reflux esophagitis and are usually associated with deep esophageal ulcers or severe diffuse esophagitis. Clinically important hemorrhage has been reported in 7% to 18% of patients with GERD. Esophageal perforations are very rare in the PPI era, but they can result in mediastinitis and can be fatal if they are not rapidly recognized and treated.
Peptic Esophageal Strictures
Strictures occur in 7% to 23% of patients with untreated reflux esophagitis, especially in older men. They usually evolve over many years and may be linked to the long-term use of nonsteroidal antiinflammatory drugs. The mechanism of stricture formation is complex, starting as a reversible inflammatory process with edema, cellular infiltration, and vascular congestion, progressing to deposition of connective tissue and collagen, and ending in irreversible fibrosis. With the onset of dysphagia, there is often less heartburn, reflecting the stricture’s acting as a barrier to reflux. Dysphagia is usually limit to solids, but it may progress to liquids. Unlike malignant strictures, patients with peptic strictures have a good appetite, alter their diet, and lose little weight.
Radiographically, peptic strictures are smooth-walled, tapered, circumferential narrowings in the lower esophagus, which are usually less than 1 cm long, but occasionally they extend to 8 cm in length. In these unusual cases, the clinician should suspect a predisposing condition, such as the Zollinger-Ellison syndrome, superimposed pill esophagitis, or prolonged nasogastric intubation. A stricture in the middle to upper esophagus should raise the suspicion of Barrett esophagus or malignant disease. Although once controversial, most data today suggest that a Schatzki ring is a forme fruste of an early peptic stricture. In all cases, the nature of a peptic stricture needs to be confirmed by endoscopy with biopsies because some patients may have Barrett esophagus or unsuspected cancer.
The clinical course of reflux esophagitis depends to a great extent on whether the patient has erosive or nonerosive GERD on initial presentation. Furthermore, patients tend not to cross over from one group to another unless they are treated medically or surgically: in follow-up ranging from 6 months to more than 5 years, only 15% of patients with nonerosive disease evolved over time to having esophagitis or complications of GERD.
Nonerosive Acid Reflux Disease
Although early studies from tertiary referral centers suggested that nearly half of patients with GERD had esophagitis, studies carried out in community practices reveal that up to 70% of the patients with GERD had a normal endoscopic examination. Furthermore, another community-based study of antacid users found that 53% of patients with GERD had nonerosive disease, and two thirds of the remaining had only minimal erosive changes at endoscopy. Endoscopy-negative patients with GERD are more likely to be female, younger, thin, and without hiatal hernia. Despite their mild mucosal damage, these patients demonstrate a chronic pattern of symptoms with periods of exacerbation and remission.
Nonerosive GERD is suspected by the presence of typical reflux symptoms with a normal endoscopic examination and is confirmed by the patient’s response to antisecretory therapy. When performed, 24-hour esophageal pH monitoring identifies three distinct subset of patients with nonerosive disease. First, there are the patients with abnormal acid exposure time who are usually responsive to antisecretory therapy. Second are the patients with normal reflux parameters but a good relationship between acid reflux episodes and symptoms. This group represents 30% to 50% of patients with nonerosive GERD and has “functional heartburn.” These patients probably have heightened esophageal sensitivity to acid and are less likely to respond to antireflux therapy. The third group is characterized by normal acid exposure times and poor symptom correlation. Despite sometimes having classical reflux symptoms, other diseases such as achalasia, gastroparesis, bile reflux, or functional dyspepsia are the cause of their symptoms. Overall, patients with nonerosive GERD do not respond to antireflux treatments as well as do patients with erosive GERD, probably because these three subsets are not carefully defined before treatment.
Erosive Acid Reflux Disease
The clinical course of patients with erosive esophagitis is more predictable and is associated with complications of GERD. Controlled studies have shown that in the absence of ongoing maintenance therapy, up to 85% of patients with erosive GERD will have a relapse within 6 months, and the relapse rate is highest in those with the more severe grades of esophagitis. This observation, however, should not prevent at least one attempt to withdraw medication, because 20% of patients remain in remission for up to 1 year, especially those with milder esophagitis grades. Although the natural history of untreated erosive GERD is well studied, two European studies suggest that these patients are more prone to reflux complications. In a Finnish study, 20 patients with erosive GERD treated with lifestyle changes, antacids, and prokinetic drugs were followed up for a median of 19 years. Fourteen patients continued to have erosions, and 6 new cases of Barrett esophagus were detected. Likewise, a large retrospective European study with 6.5 years of follow-up found a high rate of complications (21%) including 13 esophageal ulcers, 15 with strictures, and 45 patients with Barrett epithelium. However, these data must be contrasted with other studies in which no patients with erosive esophagitis developed Barrett esophagus in a 2-year trial in the
DIAGNOSTIC EVALUATION
Many tests are available for evaluating patients with suspected GERD. These tests are often unnecessary because the classical symptoms of heartburn and acid regurgitation are sufficiently specific to identify reflux disease and to begin medical treatment. However, this may not always be the case, and the clinician must decide which test to choose to arrive at a diagnosis in a reliable, timely, and cost-effective manner, depending on the information desired.
The simplest and most definitive method for diagnosing GERD and assessing its relation to symptoms (either classical or atypical) is the empiric trial of acid suppression. Unlike other tests that only suggest an association (e.g., esophagitis at endoscopy or positive symptom index on pH testing), the response to antireflux therapy ensures a cause-and-effect relationship between GERD and symptoms. Therefore, it has become the “first” test used in patients with classical or atypical reflux symptoms without “alarm” complaints. The popularity of this approach was aided by the introduction of the PPIs, which, unlike the histamine 2 receptor antagonists (H 2RAs), could drastically reduce the amount of acid reflux into the esophagus. Symptoms usually respond to a PPI trial in 7 to 14 days. If symptoms disappear with therapy and then return when the medication is stopped, GERD may be assumed.
In the reported empiric trials with heartburn, the initial dose of PPI was high (e.g., omeprazole 40 to 80 mg/d) and was given for not less than 14 days. A positive response is defined as at least 50% improvement in heartburn. Using this approach, the PPI empiric trial had a sensitivity of 68% to 83% for determining the presence of GERD. Empiric trials using a 2- to 4-month regimen of PPIs taken twice a day also are commonly used in patients with suspected GERD-associated asthma and GERD complaints related to the ear, nose and throat.
An empiric trial of PPIs for diagnosing GERD has many advantages. The test is office based, is easily performed, is relatively inexpensive, is available to all physicians, and avoids many needless procedures. Disadvantages are few, including a placebo response and uncertain symptomatic end point if symptoms do not resolve totally with extended treatment.
Extraesophageal Manifestations
It has been suggested that GER may be the cause of a wide spectrum of conditions including noncardiac chest pain, asthma, posterior laryngitis, chronic cough, recurrent pneumonitis, and even dental erosion. Some of these patients have classical reflux symptoms, but many are “silent refluxers,” contributing to problems in making the diagnosis. Furthermore, it may be difficult to establish a causal relationship even if GER can be documented by testing (e.g., pH studies), because patients may simply have two common diseases without a cause-and-effect relationship.
Chest Pain
GER-related chest pain may mimic angina pectoris. The chest pain is usually described as squeezing or burning, substernal in location, and radiating to the back, neck, jaw, or arm. It often is worse after meals, awakens the patient from sleep, and may worsen during periods of emotional stress. Heavy exercise, even treadmill testing, may provoke
Asthma and Other Pulmonary Diseases
The association of GERD and pulmonary diseases was recognized by Sir William Osler, who recommended that asthmatic patients should “learn to take their large daily meal at noon to avoid nighttime asthma which occurred if they ate a full supper.” More recent studies suggest the coexistence of the two diseases in up to 80% of asthmatic patients, irrespective of the use of bronchodilators. GERD should be considered in asthmatic patients who present in adulthood, those without an intrinsic component, and those not responding to bronchodilators or steroids. Up to 30% of patients with GERD-related asthma have no other esophageal complaints. Other pulmonary diseases associated with GERD include aspiration pneumonia, interstitial pulmonary fibrosis, chronic bronchitis, bronchiectasis, and possibly cystic fibrosis, neonatal bronchopulmonary dysplasia, and sudden infant death syndrome. Proposed mechanisms of reflux-induced asthma are either aspiration of gastric contents into the lungs with secondary bronchospasm or activation of a vagal reflex from the esophagus to the lungs causing bronchoconstriction. Animal and human studies report bronchoconstriction after esophageal acidification, but the response tends to be mild and unpredictable. In contrast, intratracheal infusion of even small amounts of acid induces profound and reproducible bronchospasm in cats. The reflux of acid into the trachea as compared with the esophagus alone predictably caused marked changes in peak expiratory flow rates in asthmatic patients. Although either mechanism may be responsible for reflux-induced asthma, most patients probably suffer from intermittent microaspiration.
Ear, Nose, and Throat Diseases
GERD may be associated with a variety of laryngeal conditions and symptoms, of which reflux laryngitis is perhaps the most common. These patients present with hoarseness, globus sensation, frequent throat clearing, recurrent sore throat, and prolonged voice warmup. Ear, nose, and throat signs attributed to GERD include posterior laryngitis with edema and redness, vocal cord ulcers and granulomas, leukoplakia, and even carcinoma. These changes usually are limited to the posterior third of the vocal cords and interarytenoid areas, both in close proximity to the upper esophageal sphincter. GERD is the third leading cause of chronic cough (after sinus problems and asthma), accounting for 20% of cases. Dental erosion, defined as the loss of tooth structure by chemical processes not involving bacteria, can be caused by GER in healthy persons and in patients with bulimia. Despite the association between ear, nose, and throat diseases and GERD, overt esophagitis usually is absent, and most patients have only mild reflux symptoms, if any. Microaspiration of gastric contents is the most likely cause of these complaints. Animal studies find that the combination of acid and pepsin is very injurious to the larynx. Human studies report that proximal esophageal acid exposure, especially at night while sleeping, is significantly increased in patients with laryngeal symptoms and signs.
Classical Reflux Symptoms
Heartburn is the classical symptom of GERD, with patients generally reporting a burning feeling, rising from the stomach or lower chest and radiating toward the neck, throat, and occasionally the back. Usually, it occurs postprandially, particularly after large meals or the consumption of spicy foods, citrus products, fats, chocolates, and alcohol. Recumbency and bending over may exacerbate heartburn. When heartburn dominates the patients’ complaints, it has very high specificity (89%), but low sensitivity (38%) for GERD as diagnosed by abnormal 24-hour esophageal pH testing. The diagnosis of GERD usually is based on the occurrence of heartburn on 2 or more days a week, although less frequent symptoms do not preclude the disease. Although this symptom is an aid to diagnosis, the frequency and severity of heartburn do not predict the degree of esophageal damage. Heartburn is caused by acid stimulation of sensory nerve endings in the deeper layers of the esophageal epithelium. These nerve endings are normally protected by a relatively impermeable epithelium, but with epithelial changes caused by reflux, they may be stimulated by H + or spicy foods.
Other common symptoms of GERD are acid regurgitation and dysphagia. The effortless regurgitation of acidic fluid, especially after meals and exacerbated by stooping or recumbency, is highly suggestive of GERD. Among patients with daily regurgitation, the LES pressure usually is low, many have associated gastroparesis, and esophagitis is common. For these reasons, acid regurgitation may be more difficult to control medically then classical heartburn complaints. Dysphagia is reported by more than 30% of patients with GERD. It usually occurs in the setting of long-standing heartburn, with slowly progressive dysphagia primarily for solids. Weight loss is uncommon because patients have good appetites. The most common causes are a peptic stricture or Schatzki ring, but other causes include severe esophageal inflammation alone, peristaltic dysfunction, and esophageal cancer arising from Barrett esophagus.
Less common reflux-associated symptoms include water brash, odynophagia, burping, hiccups, nausea, and vomiting. Water brash is the sudden appearance in the mouth of a slightly sour or salty fluid. It is not regurgitated fluid, but rather secretions from the salivary glands in response to acid reflux. Odynophagia, pain on swallowing, can occasionally be seen with severe ulcerative esophagitis. However, its presence should raise the suspicion of an alternative cause of esophagitis, especially infections (candidiasis, herpes) or pills (tetracycline, potassium chloride, quinine, vitamin C, alendronate).
In contrast to the previously described symptomatic presentations, some patients with GERD are asymptomatic. This is particularly true in elderly patients because of decreased acidity of the reflux material or decreased pain perception. Many elderly patients present first with complications of GERD because of long-standing disease with minimal symptoms. For example, up to one third of patients with Barrett esophagus are insensitive to acid at the time of presentation.
Factors related to the Stomach:
Stomach factors (particularly stomach content's volume and certain aggressive factors found in the refluxate) are potentially important in the production of reflux esophagitis. Stomach volume is determined by the basal acid secretion rate, concomitant H pylori infection, duodenogastric reflux, and the rate of stomach emptying. Increased stomach volume not only provides more stomach contents available for reflux, but also increases the rate of transient LESRs.
Stomach Acid Secretion
The primary importance of stomach acid is indisputable in the production of reflux esophagitis, but its mechanism may involve activation of pepsin rather than direct damage from acid alone. In animal studies, acid causes minimal injury at a pH of less than 3.0, primarily by protein denaturation. However, the combination of acid and even small amounts of pepsin disrupts the mucosal barrier resulting in increased H + permeability, histological changes, and gross hemorrhage. Complementing the animal studies, a series of clinical reports showed that patients with various grades of esophagitis, including Barrett esophagus, have increased frequency and duration of esophageal exposure to Stomach refluxate of pH lower than 4. Conversely, perfusing the esophagus of animals with a pepsin solution of pH 7.5 produces minimal mucosal disruption or changes in permeability. These observations are the cornerstone of acid suppressive therapy in the treatment of GERD.
Some studies have suggested that patients with reflux, especially those responding poorly to conventional antisecretory therapy, may have higher rates of acid secretion than controls. However, most evidence finds no abnormality of Stomach acid secretion in patients with GERD. Factors that reduce Stomach acid secretion naturally, for example, concomitant infection with H pylori, especially if it is the cagA + virulent strain, may protect from the development of severe esophagitis and Barrett esophagus. H pylori infection, particularly infection with this virulent strain, is a biologic antisecretory agent that lowers Stomach acidity. It produces severe corpus gastritis and accelerates the progression to multifocal atrophic gastritis and intestinal metaplasia, with concomitant lower acid output. In addition, the bacteria produce ammonia that acts as a powerful neutralizing agent at elevated pH conditions. The corpus mucosa returns to normal when the H pylori infection is cured, increasing acid secretion and possibly contributing to the reports of esophagitis after successful treatment of H pylori infection. The consequences of long-term normalization of parietal cell function and return to higher intragastric acidity is unknown, but they could promote the development of more severe GERD, Barrett esophagus, and adenocarcinoma in Western populations.
Duodenogastric Reflux
Bile acids have been implicated in the development of esophagitis, especially in the presence of increased duodenogastric reflux. Studies in animals demonstrate that conjugated bile acids produce their greatest injury in the presence of acid and pepsin, whereas trypsin, deconjugated bile salts, are more damaging in the absence of acid. Several surgical reports have suggested that duodenogastric reflux into the esophagus is frequent and may predispose to complications of GERD. However, accurate measurement of duodenogastric reflux is difficult. Duodenogastric reflux may be indirectly estimated by ambulatory pH studies using an esophageal pH of less than 7 to indicate alkaline reflux. However, the reliability of this indirect marker is now questioned by newer techniques, which either spectrophotometrically measure bilirubin, the most common pigment in bile, or measure esophageal impedance of the flow of liquids and gases independent of pH. These studies show that acid reflux and bile reflux increase together across the spectrum of GERD, making it nearly impossible to incriminate one agent over the other in the development of esophagitis. In addition, aggressive acid suppression with proton pump inhibitors (PPIs) decreases both acid and duodenogastric reflux probably by decreasing the volume of Stomach contents available to reflux into the esophagus. Finally, the absence of membrane microvesiculation and intracellular bile deposits in human esophageal biopsies, two distinctive morphologic features of experimental acid-bile salt injury, also argue against an important role for bile salts in GERD.
Delayed Stomach Emptying
The importance of delayed Stomach emptying in the pathogenesis of GERD is controversial. Early studies observed a delay in the Stomach emptying of solids in up to 50% of patients with reflux. More recent studies found only a 6% to 38% rate of delayed Stomach emptying, regardless of the severity of the esophagitis. Nevertheless, delayed Stomach emptying may be a major factor contributing to GERD in some groups, such as diabetic patients with autonomic peripheral neuropathy.
Associated Conditions
Certain medical and surgical conditions can predispose a person to GERD. The most common is pregnancy; 30% to 50% of pregnant women complain of heartburn, especially in the first trimester. Pregnancy increases the risk for reflux by the relaxing effects of circulating estrogens and progesterones on LES pressure. Although symptoms may be severe, esophagitis is uncommon, and this type of “situational” GERD is cured with childbirth.
Up to 90% of patients with scleroderma have GERD as the result of smooth muscle fibrosis causing low LES pressure and weak or absent peristalsis. Severe disease is common; up to 70% of patients have esophagitis, many have peptic strictures, and Barrett esophagus and carcinoma of the esophagus have been reported.
Unlike the previous two conditions that are characterized by LES dysfunction, hypersecretion of acid and increased Stomach volume are the major factors causing GERD in patients with the Zollinger-Ellison syndrome. In these patients, the esophagitis and complications may be more difficult to treat than the ulcer disease. After Heller myotomy, 10% to 20% of patients may develop GERD. Finally, prolonged nasogastric intubation may contribute to the development of reflux esophagitis, in part because acid tracks orad along the tube and because the tube mechanically interferes with LES barrier function.
Esophageal Acid Clearance
The second tier against reflux damage is esophageal acid clearance. Reflux events determine the frequency and extent that gastric contents enter the esophagus, but esophageal acid clearance time determines the duration the mucosa is exposed to acid and probably the severity of acid damage. Esophageal acid clearance involves two related but separate processes: volume clearance, which is the actual removal of the reflux material from the esophagus, and acid clearance, which is the restoration of normal pH in the esophagus after acid exposure through titration with base, rather than true removal of the refluxed material.
Volume Clearance
Esophageal peristalsis operates to clear the acid volume in both the upright and supine positions, but it is inoperative during deep rapid eye movement sleep. Primary peristalsis is elicited by swallowing, which occurs with a frequency of once per minute in awake subjects, regardless of whether reflux occurs. Secondary peristalsis, initiated by esophageal distention from acid reflux, is much less effective in promoting clearance of refluxate, thus offering only an ancillary protective role. Peristaltic dysfunction, that is, failed peristaltic contractions and hypotensive (<30 style="font-style: italic;">Salivary and Esophageal Gland Secretions
Saliva is the second essential factor required for normal esophageal clearance of acid. Saliva has a pH of 6.4 to 7.8 and therefore is a weak base compared with the acidic gastric contents. The high rate of spontaneous swallowing results in saliva production of approximately 0.5 mL per minute. Although saliva is ineffective in neutralizing large volumes of acid (5 to 10 mL), it can neutralize small residual amounts of acid remaining in the esophagus after the volume of refluxed material has been cleared by several peristaltic contractions The importance of swallowed saliva is supported by findings that increased salivation induced by oral lozenges or bethanechol is associated with a significant decrease in acid clearance time. In contrast, suction aspiration of saliva is accompanied by a marked prolongation of esophageal clearance, despite the presence of normal peristaltic contractions. Physiological or pathological compromises of salivation may contribute to GERD. Diminished salivation during sleep explains why nocturnal reflux episodes are associated with markedly prolonged acid clearance times. Similarly, chronic xerostomia is associated with prolonged esophageal acid exposure and esophagitis. Cigarette smoking may promote GER. This was originally attributed to the effects of nicotine on lowering LES pressure, but more recent studies suggest that cigarette smokers have hyposalivation, which may also prolong esophageal acid clearance. Finally, the esophagosalivary reflex may be impaired in patients with reflux esophagitis. This is a vasovagal reflex demonstrated by perfusing acid into the esophagus, thereby stimulating increased salivation. This reflex may explain the symptoms of water brash (copious salivation) observed in some patients with reflux disease. The esophagosalivary reflex is very active in healthy persons, with a doubling or tripling of the salivary flow rate on exposure to acid. However, this reflex is diminished in patients with esophagitis and in those with strictures. In addition to the role of saliva, dilution and neutralization of residual acid are achieved by the aqueous bicarbonate (HCO 3 -)-rich secretions of the esophageal submucosal glands. These glands have been identified in the opossum as well as in the human esophagus. Reflux of acid into the esophageal lumen stimulates these glands and helps to neutralize the acid, even if swallowing does not occur.
Tissue Resistance
Although clearance mechanisms minimize acid contact time with the epithelium, even healthy persons may have their esophagus exposed to acid 1 to 2 hours during the day and sometimes at night. Nevertheless, only a few persons experience symptomatic GER, and even fewer suffer GERD. This is the result of a third tier for esophageal defense, known as tissue resistance. Tissue resistance is not a single factor, but a group of dynamic mucosal structures and functions that interact to minimize mucosal damage from the noxious gastric refluxate. Conceptually, tissue resistance can be subdivided into preepithelial, epithelial, and postepithelial factors.
The preepithelial defense in the esophagus, in contrast to the stomach and duodenum, is poorly developed. There is neither a well-defined mucous layer nor a buffering capacity by the surface cells to secrete HCO 3 - into the unstirred water layer. This results in a lumen-to-surface pH gradient in the esophagus of 1:10, in contrast to the stomach and duodenum, where the gradient can range from 1:1000 to 1:10,000.
The epithelial defenses in the esophagus consist of both structural and functional components. Structural components include the cell membranes and intercellular junctional complexes of the esophageal mucosa. This structure is a 25- to 30-cell-thick, nonkeratinized squamous epithelium functionally divided into a proliferating basal cell layer (stratum basalis), a midzone layer of metabolically active squamous cells (stratum spinosum), and a 5- to 10-cell-thick layer of dead cells (stratum corneum). The esophageal mucosa is a relatively “tight” epithelium with resistance to ionic movement at the intercellular as well as the cellular level as the result of both tight junctions and the matrix of lipid-rich glucoconjugates in the intercellular space. The functional components of tissue resistance include the ability of the esophageal epithelium to buffer and extrude hydrogen ions (H +). Intracellular buffering is accomplished by negatively charged phosphates and proteins, as well as HCO 3 -. When the buffering capacity is exceeded and intracellular pH falls, it has the capacity actively to remove H + from the cells. This is possibly by the action of two transmembrane proteins, one a sodium (Na +)/H + exchanger and the other a Na +-dependent chloride (Cl -)/HCO 3 - exchanger. After reflux-induced cell acidification, these transporters restore the intracellular pH to neutrality by exchanging H + for extracellular Na + or by exchanging Cl - for extracellular HCO 3 -, respectively. Additionally, esophageal cells contain within their membrane a Na +-independent Cl -/HCO 3 - exchanger that extrudes HCO 3 - from the cytoplasm when the intracellular pH is too high. When the epithelial cells are no longer able to maintain intracellular pH, they lose their ability to regulate volume, edema occurs, and balloon cells develop.
The postepithelial defense is provided by the esophageal blood supply. Blood flow delivers oxygen, nutrients, and HCO 3 - and removes H + and carbon dioxide, thereby maintaining normal tissue acid-base balance. Blood flow to the esophageal mucosa increases in response to the stress of lumenal acid. Cellular injury also stimulates cell proliferation, which results in thickening of the basal cell layer of the epithelium. Unlike the stomach, in which superficial mucosal injury is repaired in hours, the esophagus repairs itself more slowly over days to weeks.
The relationship between hiatal hernia and GERD remains controversial. Mainstream opinion has shifted widely from one that virtually equated hiatal hernia with GERD to one that denied it a causal role. Currently, both epidemiologic and physiological data confirm the importance of the hiatal hernia in patients with more severe esophagitis, peptic stricture, or Barrett esophagus. Hiatal hernias, identified endoscopically or radiologically, are reported in 54% to 94% of patients with reflux esophagitis; a rate strikingly higher than in the healthy population.
The functional impact of the hiatal hernia has been clarified by elegant combined manometry and videofluoroscopic studies that show that hiatal hernia impairs LES function through several mechanisms as well as impairing esophageal clearance. Reflux is worse in patients who have a nonreducible as opposed to a reducible hiatal hernia. Nonreducing hernias are those in which the gastric rugal folds remain above the diaphragm between swallows. Furthermore, statistical modeling has revealed a significant interaction between hiatal hernia and LES pressure, such that the likelihood of GER is increased as basal LES pressure decreases, an effect that is substantially amplified by the presence of a hiatal hernia and as hernia size increases.
Displacement of the LES from the crural diaphragm into the chest reduces basal LES pressure and shortens the length of the high-pressure zone primarily because of the loss of the intra-abdominal LES segment. Both these effects are caused by the loss of the extrinsic support of the diaphragmatic crura resulting in increased GER. Hiatal hernia virtually eliminates the increase of LES pressure that occurs during straining and may increase the triggering of transient LESRs during gastric insufflation with gas. , Large, nonreducible hernias also impair esophageal acid clearance because of increased tendency for reflux to occur from the hernia sac during swallow-induced LESRs.
The origin of hiatal hernia remains unclear. Familial clustering of GERD suggests the possibilities of inherited muscle weakness in this area. Animal studies propose that reflux itself causes esophageal shortening promoting the development of a hiatal hernia. Other studies find an association with obesity and lifting of heavy weights, raising the possibilities that over time, chronic intra-abdominal stressors may weaken the esophageal hiatus and may cause the development of a hiatal hernia. This theory is attractive because it helps to reconcile the increased prevalence of hiatal hernias as the population ages.
Mechanisms of Reflux
Transient Lower Esophageal Sphincter Relaxations
This is the most common mechanism underlying GER and also accounts for the reflux of gases during belching. Transient LESRs are not associated with antecedent pharyngeal contractions, are unaccompanied by esophageal peristalsis, persist for longer periods (>10 seconds) than swallow-induced LESRs, and are always accompanied by inhibition of the crural diaphragm. Transient LESRs account for nearly all reflux episodes in healthy persons and for 50% to 80% in patients with GERD, depending on the severity of associated esophagitis. However, one study suggested that low basal LES pressure, rather than transient LESRs, may be the primary mechanism of GER in patients with nonreducible hernias. Transient LESRs are not always associated with GER. In healthy persons, about 40% to 60% of transient LESRs are accompanied by reflux episodes, compared with 60% to 70% in patients with GERD. The rate of transient LESR is increased by gastric distention, whether by gas or a meal, by stress, and, to a lesser extent, by subthreshold (for swallowing) stimulation of the pharynx. Under normal circumstances, meals are the major stimuli for transient LESRs, but the importance of specific foods is unknown. Transient LESRs are inhibited by the supine position, sleep, general anesthesia, and vagal cooling. Various drugs also impair transient LESRs including cholecystokinin A antagonists, anticholinergic drugs, morphine, somatostatin, nitric oxide inhibitors, 5-hydroxytryptamine 3 (5-HT 3) antagonists, and d-aminobutyric acid B (GABA B) agonists. Current evidence indicates that transient LESRs are mediated through vagal pathways. Gastric distention activates mechanoreceptors in the proximal stomach adjacent to the gastric cardia that send signals to the brainstem center through vagal afferent pathways. The structured sequence of motor events including LESR, inhibition of the crural diaphragm, and contractions of the esophageal body suggest that this process occurs in a programmed manner, probably controlled by a pattern generator within the vagal nuclei. The motor arm is in the vagus nerve and shares common elements with swallow-induced LESR.
Swallow-Induced Lower Esophageal Sphincter Relaxations
About 5% to 10% of reflux episodes occur during swallow-induced LESRs. Most of these episodes are associated with defective or incomplete peristalsis. During a normal swallow-induced LESR associated with normal peristalsis, reflux is uncommon because of the absence of concomitant crural diaphragm relaxation, the relatively short duration of LES relaxation (5 to 10 seconds), and the prevention of reflux by the oncoming peristaltic wave (see Reflux during swallow-induced LESR is more common in the presence of a hiatus hernia because of pooling of gastric liquids in the hernia sac and the absence of any residual diaphragmatic support during the LESR.
Hypotensive Lower Esophageal Sphincter Pressure
Stress reflux and free reflux are two mechanisms by which GER can be associated with diminished LES. Stress reflux results when a relatively hypotensive LES is overcome and is “blown open” by an abrupt increase in intra-abdominal pressure from coughing, straining, or bending. Stress reflux is unlikely when the LES pressure is greater than 10 mm Hg. Free reflux is characterized by a fall in intraesophageal pH without an identifiable change in intragastric pressure, and it usually occurs when the LES pressure is 0 to 4 mm Hg. Reflux as the result of low or absent LES pressure is uncommon. It is found mostly in patients with severe esophagitis, in whom it may account for up to 23% of reflux episodes, and rarely in patients without endoscopic evidence of esophagitis. The mechanisms of a low LES pressure are poorly understood. The presence of a hiatus hernia reduces LES pressure because the intrinsic support of the crural diaphragm is lost. Some LES weakness may be secondary to impairment of the excitatory cholinergic pathways to the LES as a result of esophagitis. Induction of experimental esophagitis in cats affects the release of acetylcholine and lowers LES pressures; changes that are reversible on healing of the esophagitis. However, healing of esophagitis in humans is rarely accompanied by an increase in LES pressure.
PATHOPHYSIOLOGY
The pathophysiology of GERD is complex and results from an imbalance between defensive factors protecting the esophagus (antireflux barriers, esophageal acid clearance, tissue resistance) and aggressive factors from the stomach contents (gastric acidity and volume and duodenal contents). The intermittent nature of symptoms and esophagitis in many patients suggests that the aggressive and defensive forces are part of a delicately balanced system.
Antireflux Barriers
The first tier of the three-tiered esophageal defense against acid damage consists of the antireflux barriers. This is an anatomically complex region that includes the intrinsic lower esophageal sphincter (LES), the diaphragmatic crura, the intra-abdominal location of the LES, the phrenoesophageal ligaments, and the acute angle of His.
The LES is a tonically contracted segment of distal esophagus about 3 to 4 cm in length. It is the major component of the antireflux barrier and is capable of preventing reflux even when it is completely displaced from the diaphragmatic crura because of a hiatus hernia. The proximal margin of the LES is normally about 1.5 to 2.0 cm above the squamocolumnar junction, whereas the distal segment, about 2 cm in length, lies within the abdominal cavity. This location of the distal LES contributes to the maintenance of gastroesophageal competence during intra-abdominal pressure events. Resting LES pressure ranges between 10 to 30 mm Hg and includes a generous reserve capacity, because a minimal basal LES pressure in the range of 5 to 10 mm Hg usually prevents GER. The LES maintains a high-pressure zone by the intrinsic tone of its muscle and by cholinergic excitatory neurons. There is considerable diurnal variation in basal LES pressure; it is lowest after meals and highest at night. It is also influenced by certain circulating peptides and hormones, foods (particularly fat), and numerous drugs. During swallowing, LES relaxation (LESR) occurs for 5 to 10 seconds, thus permitting esophageal peristalsis to sweep the swallowed bolus into the stomach.
Anatomically, the LES lies within the hiatus created by the right crus of the diaphragm, and it is anchored by the phrenoesophageal ligaments, which inserts at about the level of the squamocolumnar junction . Developmentally, the crural diaphragm arises from the dorsal mesentery of the esophagus and is innervated separately from the costal part of the diaphragm. It is inhibited by esophageal distention, during vomiting, and in association with transient LESRs, but not during swallowing. The crural diaphragm provides extrinsic squeeze to the intrinsic LES, contributing to resting pressure during inspiration and also augmenting LES pressure during periods of increased abdominal pressure such as coughing, sneezing, or bending. Crural contractions impose rhythmic pressure increases of about 5 to 10 mm Hg on the LES pressure recording. During deep inspirations and some periods of increased abdominal straining, these changes may reach 50 to 150 mm Hg.
The oblique entrance of the esophagus into the stomach creates a sharp angle on the greater curve aspect of the gastroesophageal junction, the angle of His. This angle has been shown in cadavers to create a flap valve effect that contributes to gastroesophageal junction competency.